 Español
Español UK (English)
UK (English) Deutsch
Deutsch Italiano
Italiano Русский
Русский Français
Français
Forget your password?
Need for Early Diagnosis

Need for Early Diagnosis
The signs and symptoms of CLN2 disease go beyond epilepsy
Yet children are often diagnosed with epilepsy without a further work-up for CLN2
- Average age at diagnosis is 5 years—well into the neurodegenerative decline of CLN2 disease
- Diagnosis of CLN2 disease can be delayed because1,2:
- Initial symptoms are non-specific
- CLN2 disease progression can be mistaken as side effects from anti-epileptic drugs
- Early diagnosis enables access to CLN2-specific clinical care and social support, which may positively impact outcomes and quality of life of the child and the family
- Earlier diagnosis of CLN2 disease is crucial to parental awareness as genetic carriers and reinforces the importance of family planning3
- Delays in diagnosis can be accompanied by exhaustive assessments and misdiagnoses before a definitive diagnosis is confirmed
Diagnosis of CLN2 disease is delayed an average of 2 years from first observed seizure at age 3.
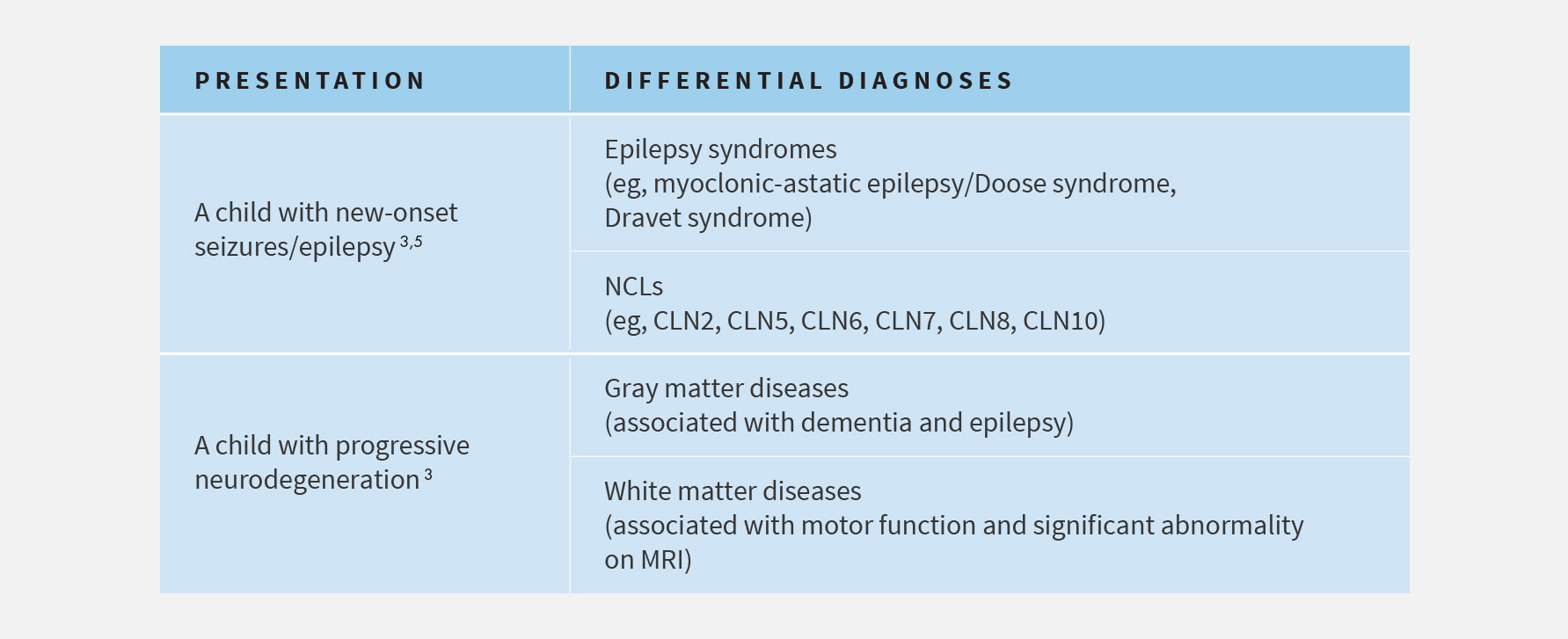
CLN2 disease is often initially misdiagnosed, delaying accurate diagnosis
Early in the progression of CLN2 disease3,4:
- Since seizures and myoclonus are the most prominent symptom, syndromes where myoclonus is common (e.g. focal epilepsy; myoclonic epilepsy syndromes/myoclonic astatic epilepsies, like Doose syndrome, Dravet syndrome, Lennox-Gastaut syndrome; or other epilepsy syndromes) are often suspected
Later in the progression of CLN2 disease3:
- As the disease progresses and psychomotor regression and functional loss become more prominent, other progressive paediatric brain disorders may be suspected (e.g. inflammation/infections, tumours, mitochondrial disorders, and other lysosomal storage diseases, including other NCL types)
References: 1. Fietz M, Giugliani R, AlSayed M, et al. Expert recommendations for the laboratory diagnosis of neuronal ceroid lipofuscinosis type 2 (CLN2 disease): diagnostic algorithm and best practice guidelines for a timely diagnosis. Poster session presented at: The 12th Annual WORLD Symposium; February – March 2016; San Diego, CA. 2. Williams RE, Adams HR, Blohm M, et al. Expert opinion on the management of CLN2 disease. Poster session presented at: The 12th Annual WORLD Symposium; February – March 2016; San Diego, CA. 3. Chang M, Cooper JD, Davidson BL, et al. CLN2. In: Mole S, Williams R, and Goebel H, eds. The neuronal ceroid lipofuscinoses (Batten Disease). 2nd ed. Oxford, United Kingdom: Oxford University Press; 2011:80-109. 4. Pérez-Poyato MS, Marfa MP, Abizanda IF, et al. Late infantile neuronal ceroid lipofuscinosis: mutations in the CLN2 gene and clinical course in Spanish patients. J Child Neurol. 2013;28:470-478. 5. Mole SE, Williams RE, and Goebel HH. Correlations between genotype, ultrastructural morphology and clinical phenotype in the neuronal ceroid lipofuscinoses. Neurogenetics. 2005;6:107-126.
